Teachers in early years education can be at risk of suffering musculoskeletal problems due to factors like regularly stooping to interact with young children, but there are practical ways of reducing the risk of pain and injury.
Features
Getting educated on musculoskeletal health
By
on 11 October 2022
There are over 20,000 primary schools in the UK, with a workforce of over 300,000 teachers and teaching assistants. There are also thousands of supply staff who work as temporary teachers and teaching assistants in primary schools and a huge number of people working in other early years education and childcare settings, like nurseries.
People who work with, come into contact with or simply talk to teachers and nursery staff may have heard anecdotal reports about those working in childcare and education workplaces suffering musculoskeletal disorders (MSDs). Any adult who has attended a parent-teacher evening in a setting like a primary school may also appreciate the discomfort that could be experienced by a teacher or nursery worker forced to sit on tiny children’s chairs, bend over low tables or kneel on the floor when teaching and interacting with the small children in their charge.
 Lorna Taylor is the founder of Jolly Back, a consultancy that provides ergonomics solutions to protect the musculoskeletal health of teachers and support staff in early years education
Lorna Taylor is the founder of Jolly Back, a consultancy that provides ergonomics solutions to protect the musculoskeletal health of teachers and support staff in early years education
However, although work in low-level ‘child height’ environments in early years education poses a number of musculoskeletal risks to teachers and nursery staff, often employers in charge of primary schools and nurseries – and the teachers themselves – have a poor understanding of how approaches like good ergonomic design of the school and its furniture, good teacher posture and the safe moving, lifting and handling of items like play equipment and young children can help ensure the musculoskeletal health of teachers.
There are a variety of reasons for this lack of focus on protecting the musculoskeletal health of teaching staff in early years education.
For example, the primary focus of education settings is most often the needs of children and awareness of MSDs within the education sector (during teacher training, while teachers are at work and amongst school leadership) is low.
As well as limited understanding among school leaders and teachers of the importance of healthy working practices to prevent MSDs in teaching staff, there may be budget restrictions preventing schools from investing in measures like teacher training on good ergonomics and the purchase of suitable ergonomic equipment, such as low-level seating to enable teachers to work in comfort at ‘child height’. Other factors include the pressure to achieve pupil academic targets preventing school leaders and teachers from dedicating adequate time and resources to reducing MSD risks to the workforce.
However, research has shown that supporting good musculoskeletal health underpins a person’s ability to live and work well. Good musculoskeletal health is also fundamental to healthy ageing, quality of life and maintaining independence beyond working years.
Therefore, if the early years education sector takes appropriate steps to protect the musculoskeletal health of its workforce, there will be benefits to teachers’ overall and long-term health. And, because research has shown there is a positive association between teacher wellbeing in general and pupil performance, supporting the musculoskeletal health of primary school teachers should also help to improve the quality of education they provide to pupils.
 Research suggests there is positive association between teacher wellbeing and pupil performance. Photograph: iStock
Research suggests there is positive association between teacher wellbeing and pupil performance. Photograph: iStock
Studies show complaints about MSDs are frequently high among education sector workers globally. For example, one 2011 study estimated that the prevalence of self-reported MSDs among schoolteachers ranged between 39 per cent and 95 per cent.
Meanwhile, a 2011 questionnaire carried out by Jolly Back for the UK education unions Voice (now part of Community) and the National Union of Teachers found that 82 per cent of early years teachers and teaching assistants had experienced work-related MSDs at least once a week. However, only eight per cent had officially reported the symptoms to their employer.
However, although the direct and indirect costs of work-related MSDs to individuals, society (including healthcare systems) and organisations are vast, MSDs are preventable.
To prevent MSDs, those in charge of early years education settings need to take a holistic and integrated approach to protecting the musculoskeletal health of teachers, teaching assistants and nursery workers.
In essence, this means identifying the MSD hazards and risks teachers may be exposed to, developing a culture of MSD prevention in schools and educating teaching staff about how to reduce MSD risks to themselves and maintain good musculoskeletal health more widely.
School leaders need to take an integrated, collaborative approach to managing MSD risks to teachers in early years education. This means consulting and involving teachers on ways of managing the risks – as they may have good ideas about the problems and the most appropriate solutions. It also means ensuring teachers have the necessary information, training and (where practical) equipment to minimise the MSD risks they face.
Risk factors and the effects of MSDs in early years and primary teachers
MSDs affect the body’s bones, muscles, joints, ligaments/tendons, and nerves. The symptoms depend on the pathophysiological mechanisms of the structures affected but commonly include pain, fatigue, stiffness and restricted joint movement, sensory loss and numbness (including sciatica) and localised swelling.
Low back pain, neck and upper limb strain and lower limb discomfort among primary and early years teachers can be caused or exacerbated by work-related activities. Common causes include:
- Uncomfortable working postures – including sitting on children’s chairs, bending over tables, kneeling, prolonged standing, prolonged sitting and when using display screen equipment (DSE), like desktop computers and laptops. There may also be MSD risks from home working, such as the poor set-up of home computer workstations
- Awkwardly lifting and moving equipment and/or young children – during classroom activities, outdoor play, PE or transporting books
- Psychosocial issues – including workload, mental health at work, job demands, job satisfaction, conflicts at work, work-related stress, and work-life balance.
MSDs experienced by educators and associated with long-term health conditions (for example, pain, joint stiffness and fatigue with rheumatoid arthritis, osteoarthritis, systemic lupus, fibromyalgia, osteoporosis and ankylosing spondylitis) can also be exacerbated by low-level working, such as bending over low-level children’s desks.
Other MSD risk factors faced by early years and primary teachers include:
- Physical inactivity – regular and appropriate physical activity maintains and improves the strength and flexibility of the body’s muscles and joints; improves circulation and associated joint and muscle nutrition; maintains and improves balance to reduce the risk of falls; and improves emotional wellbeing: all of which contribute to musculoskeletal health. In fact, studies show that increased levels of physical exercise in educators (for example, teachers) are associated with a lower incidence of MSD in the upper body. Also, educators who increase the amount of exercise they undertake show a decrease in overall MSDs.
- Unhealthy working environment – a healthy workplace design and physical environment for the musculoskeletal health of teachers incorporates ergonomics, movement, areas for rest and considers noise, lighting, temperature and air quality. However, there is a particular challenge in simultaneously meeting the ergonomic requirements of adult workers and the learning needs of children, especially in low, ‘child-height’ environments. For example, teachers may sit at a child’s chair and desk to plan or mark work simply because they lack knowledge about the ergonomic risks of using unsuitable seating and workstations or because an adult-sized workstation is not immediately available. Studies have shown that in education environments where there is higher “perception of inappropriate infrastructures” (including noise, lighting, temperature, cleaning, ventilation, size and furniture), this is significantly associated with higher MSD reporting in elementary teachers.
- Older age – increased length of employment is a strong predictor of increased MSDs in teachers. Also, teachers are working longer as retirement ages are increased, which may further increase the risk of MSDs. In addition, MSDs can begin in young workers (like teachers) but the cumulative effects only emerge later in life.
- High body mass index – being overweight increases strain on the body’s musculoskeletal system and being obese increases the risk of developing osteoarthritis of the knee. Maintaining a healthy weight and a balanced approach to diet and nutrition helps the body to repair and maintains good bone heath, both of which help to prevent osteoporosis (and the risk of fractures) in later life.
- Vitamin D and calcium deficiency – adequate Vitamin D and calcium are required for bone health. Deficiency of either of these can result in reduced bone mineral density, which increases the risk of fractures from falls (one of the most serious musculoskeletal problems in the older population)
- Smoking – in the general population, smokers and ex-smokers experience
60 per cent more pain in the back, neck and legs and a 114 per cent increase in disabling lower back pain. Smoking reduces bone mineral density, particularly among post-menopausal women. It is associated with more bone fractures and slower healing and associated with up to a 40 per cent increase in the risk of hip fractures among men. Studies show evidence there is a higher incidence of MSDs associated with smoking in teachers.
 After identifying the hazards, the assessor should consider how likely it is that MSD harm will occur, and then seek to eliminate or reduce the risks. Photograph: iStock
After identifying the hazards, the assessor should consider how likely it is that MSD harm will occur, and then seek to eliminate or reduce the risks. Photograph: iStock
MSDs can develop quickly or build slowly over time. Once developed they can adversely affect many aspects of life, including work and leisure activities, an individual’s ability to take care of their mental and physical health and the ability to drive. They can also lead to absence from work.
Mental and physical health are intertwined and MSDs and mental ill health frequently co-exist. People with depression are at a greater risk of developing back pain, depression is four times more likely in people with persistent back pain and living with MSD pain can lead to feelings of anxiety and depression. Mental health also impacts a person’s ability to cope with and recover from MSDs.
The good news is the majority of MSDs caused or aggravated by work can be prevented through measures like suitable assessment and control of the risks, commitment by school leaders and teacher participation in identifying and reducing the risks.
Also, if symptoms of MSDs already exist among teaching staff, they can often be eased and many people will fully recover if there is early intervention by their employer, suitable medical treatment is arranged or provided and education leaders take practical action to eliminate or reduce the musculoskeletal health risks in their school.
Other benefits from managing MSD risks include:
- Fewer injuries to early years and primary teachers
- Reduced risk of work-related ill health and sickness absence
- Improved employee morale and reduced stress
- Improved staffing levels, attendance and productivity
- Improved professional care and teaching to children.
Managing MSD risks in the education workforce
Working with children is a physically and emotionally demanding role. Numerous inter-relating factors contribute to musculoskeletal health in early years and primary teachers.
Risk assessment is about identifying and taking sensible measures to control risks in the workplace. The aim should be to reduce the risk of someone being injured (an employee, visitor or child) to as low as reasonably practicable.
A hazard is something which can cause harm. A risk is the chance, however large or small, that a hazard could cause harm.
As when seeking to manage any health and safety risk, risk assessments for MSDs in early years and primary education should be carried out by someone who:
- Is competent to do so (has the right skills, knowledge and experience)
- Involves workers and their representatives in the process
- Understands when specialist help or advice may be needed.
Identify MSD hazards
The assessor should look for hazards which may result in harm to teachers when working with children. Teaching staff, or their representatives, can give first-hand experience of what happens in practice. However, it is also important to consult those who only work with children occasionally.
Hazard mapping and body mapping – where teachers highlight possible MSD hazards and risks in the school and during teaching and other activities, like PE classes, and indicate areas of the body where MSD pain is being experienced – can help in identifying hazards, risks and solutions. The main areas to consider are the working environment, the work tasks and the musculoskeletal, mental and general health and wellbeing of the teaching staff.
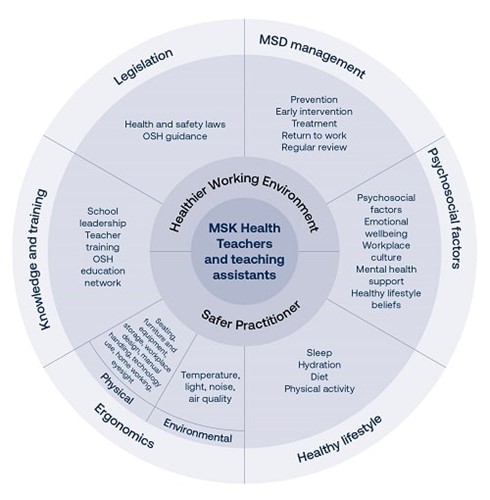 Wheel: Musculoskeletal Health for Teachers and Teaching Assistants, created for EU-OSHA Healthy Workplaces: Lighten the Load 2020-2022 campaign © Lorna Taylor
Wheel: Musculoskeletal Health for Teachers and Teaching Assistants, created for EU-OSHA Healthy Workplaces: Lighten the Load 2020-2022 campaign © Lorna Taylor
Who might be harmed?
Next, the assessor should identify who might be harmed and how. This will usually be the teacher or teaching assistant, but it might also include children or visitors. Consideration should be given to groups who may be particularly at risk of MSDs, such as: new starters, employees returning to work, those with pre-existing medical conditions, new and expectant mothers or those working long hours.
Evaluate the risks
After identifying the hazards, the assessor should consider how likely it is that MSD harm will occur, and then seek to eliminate or reduce the risks. It may not always be possible to completely eliminate MSD risks but employers have a legal duty to do everything reasonably practicable to protect employees from harm. School governors also have a critical role to play in the health and safety of school staff.
Record the findings
The significant findings of the assessment should be recorded, including the MSD prevention measures that have been, or will be, adopted. The employer should consult teaching staff, and look at records and reports of MSD problems and injuries, so that any necessary changes can be made to working practices, the work environment and the equipment provided and used to further reduce the MSD risks.
Regularly review
The MSD risk assessment should be regularly reviewed in case changes are required to further reduce MSD risks – such as if teaching staff report new symptoms of MSDs. Employers should also regularly review their MSD risk management measures to ensure that any improvements in MSD management – such as a reduction in teachers’ complaints about aches and pains – are sustained in the long run.
Changes that could indicate the assessment needs to be reviewed and the risk controls might need to be updated include:
- Teachers being responsible for higher numbers of children – for example, this could mean increased time spent bending over low desks or more time spent moving, lifting and carrying classroom or PE equipment
- The introduction of new or additional children with specific moving and handling needs – for example, teachers may have to spend more time lifting and assisting pupils with mobility challenges
- The introduction of new equipment – such as heavy play equipment that needs to be moved and carried
- Changes to buildings and classrooms – such as the introduction of new computer workstations for use by teachers.
MSD prevention guidance for early years and primary teachers
The following measures can help to effectively manage the risk of MSDs in schools. They can be loosely be divided into steps to achieve a ‘healthier working environment’ and a ‘safer practitioner’ (teacher or teaching assistant etc).
Healthier working environment
Seating, furniture and equipment
- A range of safe, appropriate seating to meet the needs of practitioners should be offered – for example, a suitable ergonomic low ‘mobile’ chair can help reduce MSD risks when working with children at low heights; floor chairs are available with a cushioned back that can be placed on the floor to support the back while sitting on the floor; and height and tilt-adjustable chairs can reduce MSD risks when sitting at a full size adult desk during teaching, writing or when using computers
- The ergonomic benefits are considered when purchasing new seating, furniture and equipment for use by practitioners
- Seating, furniture and equipment is in good working order and meets health and safety requirements
- Seating, furniture and equipment is inspected and maintained at regular intervals, in line with the manufacturer’s recommendations and maintenance schedules
- Manual handling equipment is provided and used appropriately by practitioners and others – such as hand trucks to move heavy play equipment or furniture
- Unsafe equipment is removed immediately from service and reported to a named contact so it can be repaired or replaced.
Storage
Furniture and equipment are safely stored and the storage areas can be easily accessed to minimise practitioner lifting, carrying and awkward postures
Mobile storage solutions are considered and used where possible – such as dedicated trolleys for storing and moving books and children’s lunch boxes, that can be easily and safely moved by practitioners.
Workplace design
- Employees have access to adult height desks and chairs for written and computer work and access to adult height sinks for hand washing
or washing items (or can use a washing up bowl while standing) - Consideration is given to practitioners’ working postures – including providing equipment to reduce MSD risks during low, ‘child height’ working
Floors are even, unobstructed and well-lit, and doorways (including those leading to storage areas) are accessible - Children’s independence is encouraged so they access their own resources and equipment, especially at mealtimes, to reduce practitioner lifting and carrying
- Practitioners are encouraged to regularly move and/or exercise, take rest breaks and ensure they are adequately hydrated throughout the working day
- Timetabling allows as much time as possible for children to be independent (such as helping to set up their own art, play and PE lessons and activities), and for fewer room changes to reduce the need for staff to carry and move resources for education activities, like books, art materials and paper
- Employees are asked about their seating requirements and the comfort of their workstation, desk and classroom set-up
- The health and safety needs of practitioners are considered when designing new build schools and classrooms or upgrading existing facilities.
Safer practitioner
Training
- Practitioners are given regular training on the risks from poor posture and tasks like lifting equipment and children, the health benefits of good posture and back care and safe manual handling, including how to safely lift and move children in a range of situations
- Employees and volunteers who regularly use desktop computers and mobile DSE, like laptops and tablets, are provided with regular training on minimising the associated MSD risks.
Knowledge
- Teachers and teaching assistants are aware of MSD risks in their workplace and how to reduce them (in the classroom, during outdoor learning and at a computer)
- Practitioners know how to carry out routine safety checks on mobile and safety equipment (such as faulty wheels on mobile bookcases that could mean they need to use extra force to move them), and report any faults
Teaching and teaching assistants are competent and capable of doing their work in a way that is safe for them and other people - Practitioners know how to recognise and report early symptoms of MSD ill health via a clear reporting system and are encouraged to do so by school leadership.
- Healthy lifestyle advice is provided and the school leadership implement and encourage initiatives that will support both the good musculoskeletal health and general health and wellbeing of teaching staff. Good practice examples include, active travel, like cycling to work; physically active school challenges, like encouraging staff to use the stairs instead of lifts to boost physical activity and movement; providing healthy canteen food and healthy eating tips; recognition and reduction of heavy workloads that could exacerbate MSD risks, such as spending long hours at DSE workstations; and the importance of sleep for good musculoskeletal health.
If an employer needs help to reduce MSD risks at source, intervene at an early stage to support a staff member experiencing MSD symptoms that could be caused or aggravated by work and help a staff member return to work after developing an MSD, they can consult an occupational health and safety advisor.
It is also worth noting that research shows an increasing number of children and young people are experiencing MSDs – and at an earlier age – as modern lifestyles impact on their musculoskeletal health.
For example, sedentary postures, both at home and at school, insufficient physical activity and poor diet can all have a negative impact on the musculoskeletal health of children and young people.
However, those in charge of education settings like schools have a great opportunity to educate children and young people about the benefits of maintaining good musculoskeletal health. If embedded, these healthy habits will be carried forward on a life-long basis into adulthood and when entering employment, in turn reducing the prevalence of MSDs in the future population and workforce.
Therefore, school leaders should adopt a ‘whole-school’ approach to preventing MSDs and educating everyone in the school about good musculoskeletal health – both staff and children.
For children and young people, this might include measures such as highlighting how to safely use technology associated with causing MSDs, like the safe set-up of computers and laptops, and the MSD risks from prolonged sitting.
Other possible measures include providing a variety of seating in schools to suit a range of student heights; providing lockers for the safe storage of school bags to avoid the need for pupils to carry heavy bags around; and providing information to parents on protecting children’s musculoskeletal health – such as on the good ergonomic set-up of computer workstations at home.
Conclusion
Interventions to support the health of teachers, including to prevent MSDs, have positive benefits for schools in terms of outcomes like lower staff absence rates and higher staff morale and retention. However, taking steps to positively support the health and wellbeing of teachers and teaching assistants has also been shown to improve the learning experiences and educational outcomes for children and young people. Put simply, research suggests there is positive association between teacher wellbeing and pupil performance.
However, to successfully reduce the risk of MSDs to staff in early and primary years education, school leaders need to take a holistic and integrated approach. This includes taking account of all the physical, emotional and social factors that can cause or aggravate MSDs in teaching staff and children and focusing on preventing MSD risks at source – though approaches like providing good ergonomic equipment and staff training on avoiding MSD risks.
There must also be early intervention to support staff experiencing MSDs – to prevent the problem getting worse, to enable the individual to recover from the symptoms and to enable them to either remain in or return to work.
Lorna Taylor is a chartered paediatric physiotherapist working within early years and primary education settings. She is the founder of Jolly Back, a consultancy that provides ergonomics solutions to protect the musculoskeletal health of teachers and support staff in early years and primary education, paediatric therapists and others caring for young children.
Lorna is also the UK ambassador for ENETOSH (European Network for Education in Occupational Safety and Health), a European Commission-backed programme that aims to integrate safety, health and wellbeing into the European education system in order to promote a culture of prevention at individual, organisational and societal levels.
Contact her at: jollyback.com


FEATURES

5 trends to watch in the safety sector in 2025
By David Head, Draeger Safety UK on 19 March 2025
Dräger’s annual Safety and Health at Work Report provides a useful insight and snapshot into the views of employees and managers on safety in UK workplaces. This year’s report suggests employers need to increase and refine their efforts in areas such as employee mental wellbeing, more structured safety training and greater use of digital and connected safety technology.
Get a hold on HAVS, before it’s too late
By Tim Turney, Casella on 18 March 2025
Employers may need to carry out measurements of hand-arm vibration from hand-held tools and machinery to identify if workers are at risk of debilitating and permanent damage to their fingers, hands and arms, but it’s essential the measurement equipment is used in the correct way.

The UK Hearing Conservation Association: how we work to promote the protection of the nation’s hearing health
By Leah Philpott, member, UKHCA At Work Group on 14 March 2025
The UK Hearing Conservation Association is a multi-disciplinary association that strives to prevent damage to the nation’s hearing health and other noise-related health conditions through a combination of practical, evidenced and cost-effective campaigns, awareness-raising activities and best-practice advice. It is therefore a great forum for those wishing to keep abreast of the latest developments around hearing health – both in the workplace and in recreational settings.